






Managing ADRs
When confronted with an ADR, ask yourself: is this a dose-related reaction or not?Dose-related reactions are an extension of the normal pharmacology of a drug. You may have heard them being called 'Type A' reactions. For example, some drugs designed to lower blood pressure in people with hypertension can lower it too much if the dose is large enough, and cause hypotension. This is a dose-related reaction. Depending on the circumstances a dose-related reaction might be managed by:
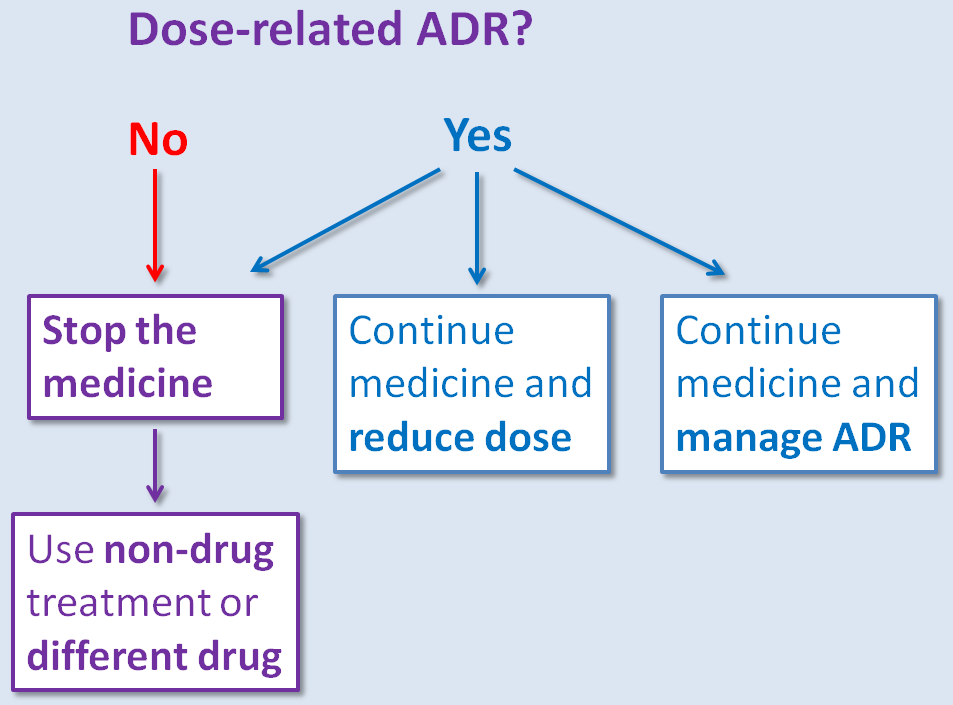
(a) Stopping the drug temporarily or permanently (e.g. a serious haemorrhage in a patient taking warfarin), or
(b) Reducing the dose (e.g. daytime sedation in a patient receiving amitriptyline for neuropathic pain), or
(c) Continuing the medicine and treating the ADR (e.g. constipation in a patient receiving morphine is usually treated with a laxative).
(b) Reducing the dose (e.g. daytime sedation in a patient receiving amitriptyline for neuropathic pain), or
(c) Continuing the medicine and treating the ADR (e.g. constipation in a patient receiving morphine is usually treated with a laxative).
ADRs that are not dose-related are more idiosyncratic and unpredictable. You might have heard these called 'Type B' reactions. Usually, the offending medicine has to be stopped in patients suffering from this type of reaction.
The diagram below summarises some basic options to consider when managing an ADR:
These options may or may not be appropriate in an individual patient depending upon the circumstances: it is not possible to generalise. Of course, how you manage a reaction in practice depends on many factors related to the patient concerned, such as:
- The severity of the reaction.
- Whether you are certain that you know which drug is responsible.
- The consequences if you stop the offending medicine. Is it safe? What other medicine could be used instead?
- Whether a dose reduction is feasible or practical.
- The ability to successfully treat the side effect.
The Type A and B classification system has been extended to include reactions that persist for a relatively long time (Type C or ‘continuing’) such as lung fibrosis with methotrexate, those that may be relatively delayed after drug exposure (Type D) such as hepatitis with flucloxacillin which can occur after the drug has been stopped, and end-of-use reactions (Type E) such as discontinuation syndromes with antidepressants.
Other classification systems have been developed such as DoTS; is the adverse reaction dose-related, time-related or does the patient have factors that make them more susceptible to developing a side effect.
Your practical knowledge about the management of ADRs increases rapidly as you gain experience, but at the beginning of your career it's appropriate to ask more senior colleagues for advice if you are not sure what to do. Some of the Information sources at the end of this tutorial may also assist you.